
Introduction
For the longest time, face aesthetics were generally understood with one basic idea: soften wrinkles, create volume or tighten skin. Botox was the symbol of this age, since it was easy to describe and easy to recognise. But now facial aesthetics expertise is moving into a much more sophisticated stage. The new revolution is not just about looking younger. It is about quantifying the face in a more objective way, organising treatments in a more exact way, improving skin biology, promoting collagen, anticipating results and even removing tiny extra skin without traditional surgery. In short, aesthetics is evolving beyond cosmetic repair to digital, biological and technology-guided facial rejuvenation. The paper discusses five important advances fuelling that change: AI-enabled facial analysis, 3D imaging and digital twins, regenerative aesthetics, energy-based collagen remodelling, and micro-coring tissue excision.


- Facial aesthetics is moving beyond wrinkles, volume, and skin tightening.
- The new focus is measurement, biology, prediction, and personalization.
- Technology now guides rejuvenation, not just cosmetic surface repair.
1. AI-powered facial analysis and treatment planning
AI-powered facial analysis employs machine learning and computer vision to analyse the face in a more structured and quantitative way. Rather than relying on the practitioner’s ‘expert eye’ alone, AI technologies can be used to assess facial symmetry, skin texture, pigmentation, redness, wrinkles, pores, volume loss, facial proportions and obvious ageing patterns. Such technologies are increasingly studied in aesthetic medicine for facial analysis, treatment planning, result prediction, documentation and patient education. It usually starts with high-resolution photos or facial scans. The software detects features of the face, including the eyes, nose, lips, cheeks, chin and jawline. It may then compare facial dimensions, measure asymmetry, assess skin quality or produce a visual map of ageing changes. Some systems can also simulate possible outcomes, allowing patients to understand what a treatment may realistically change before anything is done. In fact, AI is mostly employed as a support tool in a clinical setting and is not a replacement for a medical or aesthetic practitioner. AI can be used in consultations, before and after recording, treatment planning, skin analysis and follow-up visits. For example, a clinic might employ AI to illustrate a patient where they are losing volume, how their pigmentation has altered over time or how face balance could be affected by a medication. The chief merit here is its impartiality. Sometimes aesthetic consultations might be ambiguous, because beauty, ageing and face harmony are largely subjective. AI can bring quantifiable data to the debate. This may improve patient education, aid with treatment planning and enhance medico-legal documentation by capturing more explicitly the patient's baseline attributes and treatment goals. But AI also has fundamental limits. The better the data an AI system is trained on, the better the AI system will be. Results may be skewed or less accurate for some patients if training data lacks sufficient variety in age, sex, ethnicity, facial anatomy, and skin tone. AI simulations can potentially produce false expectations if they are presented as certain results. The face is living tissue, and ultimate results are dependent on anatomy, healing, swelling, skin quality, technique and biology. What is important to remember is that AI does not replace clinical judgement. It gives it a measurable dimension. But the future aesthetic clinic may start with a diagnostic scan rather than a mirror, and safe and ethical treatment will always depend on human experience.
2. 3D imaging, digital twins, and predictive simulation
3D imaging generates a model of the face of the patient in three dimensions. Unlike a flat snapshot, a 3D facial scan also captures depth, contour, projection, volume, and asymmetry. It is included in the concept of a digital twin as a digital model for the acquisition of the face of the patient and for the simulation of potential changes in the therapy. This is crucial since facial ageing is not just a superficial concern. You see wrinkles on the surface, but beneath are deeper changes: fat pads move, bone support changes, skin thins, and collagen declines. Gradually, the face loses its structural balance. With the 3D model the clinicians can see the face as a three-dimensional structure instead of merely a two-dimensional photograph. In aesthetic practice, 3D imaging can be used to plan fillers, rhinoplasty, facelifts, jawline contouring, chin enlargement, skin tightening, laser treatments, and long-term facial ageing studies. It can also help to compare treatment outcomes over time. Digital modelling and machine-learning-assisted planning are already used by several facial plastic surgery programmes to develop more individualised surgical plans. The most interesting usage is in predictive simulation. Before treatment, a patient may be able to see what probable changes to the cheekbones, jawline, nose, chin, lips or skin laxity might look like. This does not guarantee the result but can aid in making the consultation more visual and realistic. It is not just a matter of stating, ‘This may enhance your face balance,' but showing what that change might look like. The technology is widely utilised in advanced aesthetic and surgical surgery, but its sophistication varies. Some systems are already utilised for photography, consulting, and simulation. More advanced digital twin models with 3D imaging, AI prediction, tissue behaviour, and long-term outcome tracking are still in development. The advantages are obvious. 3D imaging can improve communication, reduce misunderstanding, help to avoid over-correction and allow for more personalised planning. It might also help patients understand why “more treatment” is not necessarily better. Sometimes the best effect is increasing the harmony of the face rather than adding volume to a specific location. The constraints are crucial as well. A simulation is not a commitment. Skin elasticity, swelling, filler behaviour, scar formation, collagen reaction, muscle mobility, and healing biology all contribute to the outcome. Current technology can offer views of possibilities but cannot forecast each biological response exactly. The crucial thing to realise is that 3D imaging is not a fancy before-and-after tool. It is part of a wider trend toward quantitative, anatomic-based, individualised aesthetic planning.
3. Regenerative aesthetics: Exosomes, polynucleotides, PRP, and cell-signalling therapies
Regenerative aesthetics is one of the most interesting and sometimes contentious fields of facial aesthetics. Traditional aesthetic treatments often involve relaxing muscles, filling wrinkles, resurfacing skin, or tightening tissue. Regenerative aesthetics looks to enhance the biological quality of the skin itself. The idea is not just to mask ageing. Its role is to affect repair, collagen signalling, hydration, inflammation management, pigmentation balance, wound healing, and overall skin quality. This is why regenerative aesthetics is often defined as a shift from “camouflage” to “tissue regeneration". The most common examples are PRP, polynucleotides and exosome-based treatments. PRP, or platelet-rich plasma, is taken from the patient’s own blood. A tiny volume of blood is drawn and spun in a centrifuge to separate and concentrate the platelet-rich plasma. Platelets also include growth factors and signalling molecules that may promote tissue repair and healing. In aesthetic dermatology, PRP is used for skin rejuvenation, acne scarring, hair restoration, wound healing assistance and occasionally as an add-on following micro-needling or laser procedures. A 2024 systematic review found evidence supporting PRP in cosmetic dermatology, particularly for skin rejuvenation, hair regrowth, wound healing and scar improvement, but also observed that treatment methodologies and trial designs vary greatly. In some markets, polynucleotides (DNA-derived compounds) are employed as injectable or topical skin stimulants. They are commonly touted for skin hydration, elasticity, texture and fine wrinkles. Some are made up of pure pieces of salmon DNA. Reviews reveal that polynucleotides may enhance skin texture, depth of wrinkles, elasticity, hydration, and facial attractiveness, but research is constantly growing, and treatment procedures are not fully standardised. Exosomes are the most publicised aspect of regenerative aesthetics. Exosomes are small extracellular vesicles that are released by cells. They can carry proteins, lipids, RNA and other signalling molecules, which is why they are being researched in tissue repair and regeneration. But the regulatory environment is really essential. The FDA has noted that there are presently no FDA-approved exosome products and items promoted with unsubstantiated claims may pose safety hazards for patients. That difference is important. PRP is autologous (from the patient’s own body) but still requires good medical skill and infection control. Polynucleotides are available in various areas, although product approval and permitted usage differ by country. Exosomes are scientifically intriguing but require rigorous supervision, as source material, manufacturing quality, sterility, dosage, stability and biological impacts are key problems. In clinical practice, regeneration treatments are typically utilised as skin quality treatments or in combination with procedures such as micro-needling, lasers, RF micro-needling or skin boosters. This combination approach is in the larger trend of ‘treatment stacking', where one treatment gives mechanical or thermal stimulation to skin, and another is designed to support repair or biological signalling. Benefits may include smoother skin texture, improved shine, improved hydration, faster recovery after treatments, collagen support and more natural-looking rejuvenation. The hazards include bruising, swelling, infection, allergic reactions, changes in pigmentation, poor technique, uneven outcomes and uncontrolled goods. The biggest problem with exosomes is that the marketing has outpaced the regulation and proof. It is important to understand is that regenerative aesthetics is not magic. It is based on wound-healing biology and cell signalling, but the evidence is spotty. PRP is routinely utilised with moderate, but inconsistent, evidence. There is more evidence emerging that polynucleotides are skin enhancers. Exosome-based goods are promising in research, but they are not FDA-authorised items and should be addressed with significant regulatory caution.
4. Energy-based collagen remodelling: RF micro-needling, ultrasound, lasers, and hybrid platforms
Energy-based collagen remodelling uses controlled injury or controlled heating to stimulate skin repair. Instead of simply filling lines or relaxing muscles, these treatments try to make the skin rebuild part of its own support structure. The major technologies are radiofrequency microneedling, microfocused ultrasound, fractional lasers, strong pulsed light and broadband light, and hybrid platforms that use different kinds of energy. Each has a different mechanism of action, but all are designed to stimulate collagen remodelling, enhance skin texture, minimise mild laxity, treat pigmentation, soften fine wrinkles and improve overall skin quality. RF micro-needling employs small needles to penetrate the skin and deliver the radio-frequency heat into deeper layers. Fractional lasers create tiny therapeutic zones that stimulate resurfacing and collagen formation. Ultrasound devices direct energy to precise depths to heat deeper tissues. Intense Pulsed Light (IPL) and BroadBand Light (BBL) use light-based energy to treat pigmentation, redness, vascular alterations and sun damage. In clinical practice, these technologies are applied for acne scars, fine lines and wrinkles, enlarged pores, skin texture, pigmentation, redness, mild laxity and photo-ageing. Some treatments are utilised as stand-alone procedures, while others are paired with injectables, skin boosters, PRP or regenerative products. In reviews, RF micro-needling has been reported to be helpful for numerous aesthetic reasons, including ageing-related wrinkles and acne scars. The result depends on device settings, patient selection, and operator expertise. The disruptive trend is not simply the devices themselves but the way they are being combined: Increasingly, modern aesthetic therapy is shifting to multilayer treatment programmes. One layer might be for pigmentation, one might stimulate collagen, one might enhance hydration, and one might help healing. This is why non-surgical facial rejuvenation is becoming more of a biological engineering approach rather than a single cosmetic procedure. These therapies can do a lot of good. Unlike surgery, they generally have minimal downtime, are capable of treating multiple skin problems simultaneously, and can provide progressive, natural-looking improvements. They also allow practitioners to treat different depths of the skin without the need for surgical incisions. But they are medical operations, not just beauty treatments. The FDA says micro-needling devices that are legally permitted have been allowed for certain uses, including enhancing the appearance of face acne scars, facial wrinkles and abdominal scars in persons age 22 or older. The FDA further points out that not all micro-needling products are approved medical devices and not all of the stated uses have been evaluated. Special attention is needed in RF microneedling. In October 2025, the FDA released a safety notification alerting concerning reports of serious problems with some uses of RF micro-needling devices, including burns, scarring, fat loss, deformity, nerve damage, and injuries needing medical or surgical intervention. The FDA further stressed that RF micro-needling is a medical procedure and should not be done at home. The evidence is strongest for some applications and weaker for others. There is clinical evidence for lasers, Intense Pulsed Light (IPL), Radiofrequency (RF) and ultrasound; however, the results are different depending on the technology, depth of treatment, skin type, surroundings, practitioner training and aftercare. Over-aggressive therapy can lead to burns, pigmentation changes, scarring, fat loss or chronic irritation. Those of darker skin types may need to take further care, as certain energy-based treatments can produce post-inflammatory hyperpigmentation (PIH) if done wrong.
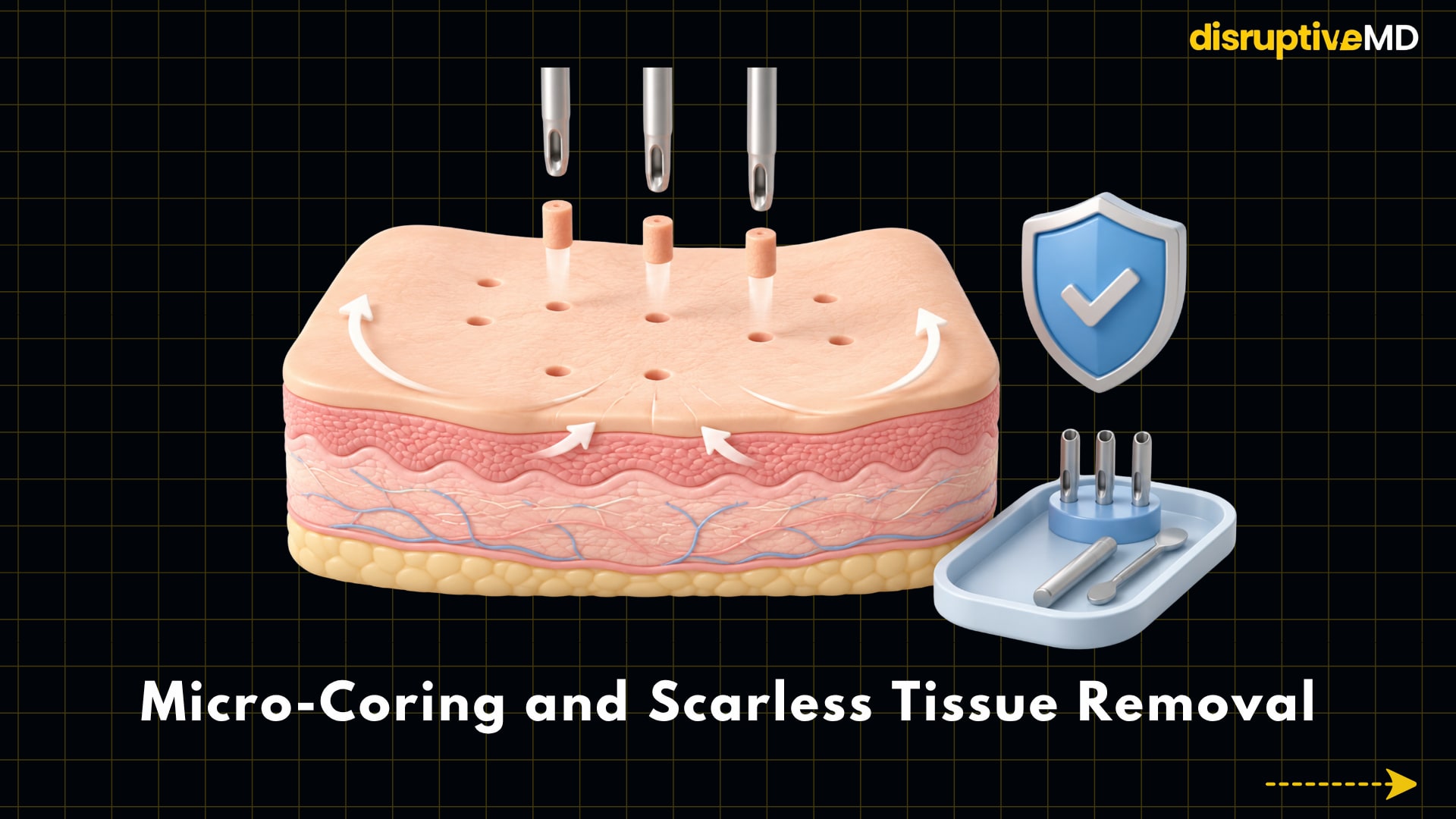
5. Micro-coring and scarless tissue removal
Micro-coring is one of the most exciting new areas in the world of facial aesthetics because it straddles non-invasive tightening and surgery. It does not merely heat the skin or promote collagen from the outside. It mechanically pulls up microscopic columns of skin through hollow needles. This method is not the same as that of lasers, ultrasound or RF micro-needling. A laser uses light energy. RF micro-needling involves needles and heat. Micro-coring removes small columns of dermal and epidermal tissue physically by using hollow needles. Then the skin around those tiny cores contracts and heals, which can improve laxity and decrease wrinkles. Micro-coring is performed in clinical practice by qualified medical specialists for selected individuals with moderate to severe wrinkles or laxity, particularly in the mid and lower face. The possible benefit is that micro-coring might give more noticeable tissue reduction than some noninvasive tightening devices, without the need for a typical facelift incision. It’s a new “middle category” of face rejuvenation. It may appeal to those who desire more than lotions and lasers or modest tightening but are not ready for surgery lifting. The constraints count. Micro-coring is not a facelift substitute. It does not move deep facial tissues, tighten the Superficial Musculoaponeurotic System (SMAS) layer, correct substantial jowling, or duplicate the outcomes of a surgical face lift. It is better understood as fractional mechanical tissue removal rather than full facial lifting surgery. Side effects may include redness, swelling, bruising, bleeding, soreness, tenderness, crusting, dryness, colour changes, infection, scarring, skin abnormalities, uneven outcomes, and anaesthetic risks. Aesthetic procedures such as laser, chemical peel, and dermabrasion that remove or harm the skin require patient selection, sterile methodology, correct aftercare, and educated providers.
The bigger picture: aesthetics is becoming more precise, biological, and personalised.
The truth behind these five advancements is not that facial aesthetics are becoming more futuristic for the sake of technology. The most profound change is that aesthetic medicine is becoming more measured, more biological and more customised. AI supports facial analysis. 3D imaging facilitates visualisation of the structure and simulates potential results. Regenerative procedures are focused on improving the quality of the tissue. Energy-based devices promote collagen remodelling. Micro-coring provides a new approach to remove small amounts of excess skin without traditional surgery. The combined use of these technologies is changing the goal of cosmetic treatment. The goal is to comprehend the face as a living structure of skin, fat, muscle, bone, blood supply, collagen, pigment, inflammation and healing biology. But the future needs to be managed cautiously. More technology does not imply better therapy. Nothing will change the best results, precise diagnosis, realistic expectations, ethical practice, safe technology, controlled products, proper training and respect for natural face harmony. The future aesthetic clinic may not start with the query, “What do you want to change?” It could start with a scan, a facial map, a biological assessment and a careful talk about what can be safely and realistically improved. That is the true Botox-beyond revolution.
References
- Al-Dhubaibi MS, Mohammed GF, Atef LM, Bahaj SS, Al-Dhubaibi AM, Bukhari AM. Artificial Intelligence in Aesthetic Medicine: Applications, Challenges, and Future Directions. J Cosmet Dermatol. 2025 Jun;24(6):e70241. doi: 10.1111/jocd.70241. PMID: 40501296; PMCID: PMC12159716.
- Chen, X., Zhou, Z., Ding, H. et al. Transforming Aesthetic Dermatology: The Role of Artificial Intelligence in Skin Health. Dermatol Ther (Heidelb) 15, 1999–2013 (2025). https://doi.org/10.1007/s13555-025-01459-2
- Yale Medicine: 3-D Planning for Facial Plastic Surgery — clinical overview of digital modeling and machine-learning-assisted planning in facial plastic surgery.
- Asubiaro J, Avajah F. Platelet-Rich Plasma in Aesthetic Dermatology: Current Evidence and Future Directions. Cureus. 2024 Aug 12;16(8):e66734. doi: 10.7759/cureus.66734. PMID: 39268288; PMCID: PMC11391108.
- Lee KWA, Chan KWL, Lee A, Lee CH, Wan J, Wong S, Yi KH. Polynucleotides in Aesthetic Medicine: A Review of Current Practices and Perceived Effectiveness. Int J Mol Sci. 2024 Jul 27;25(15):8224. doi: 10.3390/ijms25158224. PMID: 39125793; PMCID: PMC11311621.
- FDA Public Safety Notification on Exosome Products — FDA statement noting that there are currently no FDA-approved exosome products.
- FDA Microneedling Devices Guidance — FDA information on legally authorized microneedling uses and safety considerations.
- FDA Safety Communication on RF Microneedling — FDA warning on reported serious complications including burns, scarring, fat loss, disfigurement, and nerve damage.
- Shauly O, Marxen T, Menon A, Gould DJ, Miller LB, Losken A. Radiofrequency Microneedling: Technology, Devices, and Indications in the Modern Plastic Surgery Practice. Aesthet Surg J Open Forum. 2023 Nov 6;5:ojad100. doi: 10.1093/asjof/ojad100. PMID: 38887534; PMCID: PMC11181949.
- Dermal Micro-coring for the Treatment of Moderate to Severe Facial Wrinkles — clinical study evaluating micro-coring safety and efficacy for facial wrinkles.
- FDA 510(k) Premarket Notification: Cytrellis Dermal Micro-Coring System — FDA device record for the micro-coring system.
- Gfrerer L, Kilmer SL, Waibel JS, Geronemus RG, Biesman BS. Dermal Micro-coring for the Treatment of Moderate to Severe Facial Wrinkles. Plast Reconstr Surg Glob Open. 2022 Oct 17;10(10):e4547. doi: 10.1097/GOX.0000000000004547. PMID: 36262685; PMCID: PMC9575956.