
Introduction
A major challenge motivating the development of orthopaedic surgery is the high prevalence, disability and patient-specific variability of musculoskeletal disease. Musculoskeletal problems such as osteoarthritis, fractures, back pain, amputations and inflammatory joint diseases affect an estimated 171 million individuals globally, according to the World Health Organization. They are also major causes of years lived with disability. This is important because orthopedic surgery is no longer only about fixing broken bones or replacing joints, but rather about making procedures accurate, individualized, measurable and recoverable through technology.
The top 5 disruptive developments in this discipline include robotic aided joint replacement, 3D printing and patient customized surgical guides, augmented reality navigation, artificial intelligence for imaging and planning and sensor enabled implants with remote recovery monitoring. They are each changing a separate piece of the care puzzle: pre-operative planning, intra-operative accuracy, implant personalization, diagnostic decision support, and post-operative rehabilitation. The key is not whether these instruments are spectacular, but whether they improve outcomes that matter to patients: pain alleviation, function, safety, durability, recovery time, and access to care.
Why Orthopaedics Needed a Change in Technology
Orthopaedic surgery is based on anatomy, alignment and biomechanics – how bones, joints, ligaments, muscles and implants perform under strain. A few degrees of implant malposition, or a tiny error in screw placement can be critical when a joint replacement must survive years of walking, stair climbing and body weight, or when a spine screw is put near the spinal cord, nerves and blood vessels. Traditional surgery uses anatomical landmarks, X-rays, surgeon experience and mechanical instruments; these are still important but today’s technologies can also incorporate digital planning, real-time navigation and objective measurement to help minimise unwanted variance.
This is important since musculoskeletal disease is not a single problem. A young athlete with cartilage injury, an older adult with knee osteoarthritis, a trauma patient with a complex fracture, and a patient needing spine stabilization all require distinct technological solutions. The most valuable developments in orthopaedics are therefore not gadgets in isolation, but systems that assist physicians to fit the treatment, implant and rehabilitation pathway to the particular patient. Keeping safety and evidence at the centre of decision making.


- Robotic-assisted joint replacement combines three-dimensional preoperative planning with real-time computer navigation.
- The robot does not replace the surgeon; it acts as a controlled guidance system for bone preparation and implant positioning.
- Current evidence supports improved alignment precision, but better precision has not yet clearly translated into superior patient-reported outcomes.
Top 5 Innovations and What They Do
1. Robotic assisted joint replacement
Robotic-assisted joint replacement uses 3D preoperative planning with computer navigation in real time so that the surgeon may plan the cuts of the bone and the placement of the implant before the surgery and then utilize the robotic tools during the surgery to stay within that plan. Instead, the robot functions as a super-controlled guidance system that helps remove diseased bone and cartilage and helps position the replacement joint more consistently, but it does not replace the surgeon. This is most important in clinical practice for operations such as total knee arthroplasty, where alignment, soft-tissue balance and component location can influence comfort, stability and implant mechanics.
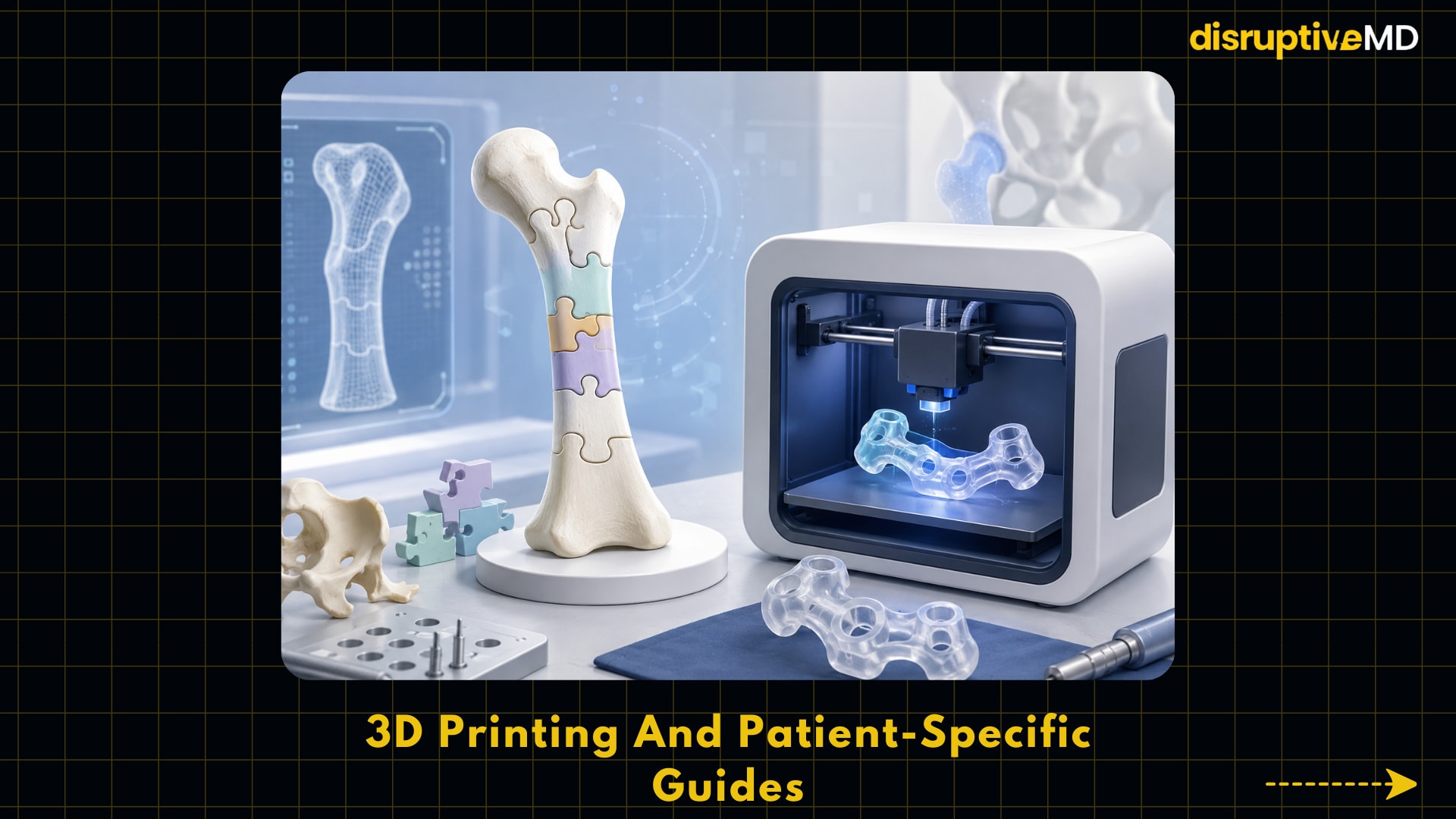
2. Patient-specific guidelines and 3D printing
Three-dimensional printing, also known as additive manufacturing, creates a device layer by layer from a digital file such as a CT scan, MRI scan or computer-aided design model. In orthopaedics, this might result in the generation of anatomical models, patient-specific cutting guides, porous implant surfaces, custom reconstruction implants, and surgical equipment. The FDA says 3D-printed medical devices include orthopedic and cranial implants and devices that are customizable to a patient’s anatomy or have complicated internal features. This is important because atypical bone loss, deformity, tumor repair, trauma and revision surgery often do not suit standardized implant shapes.
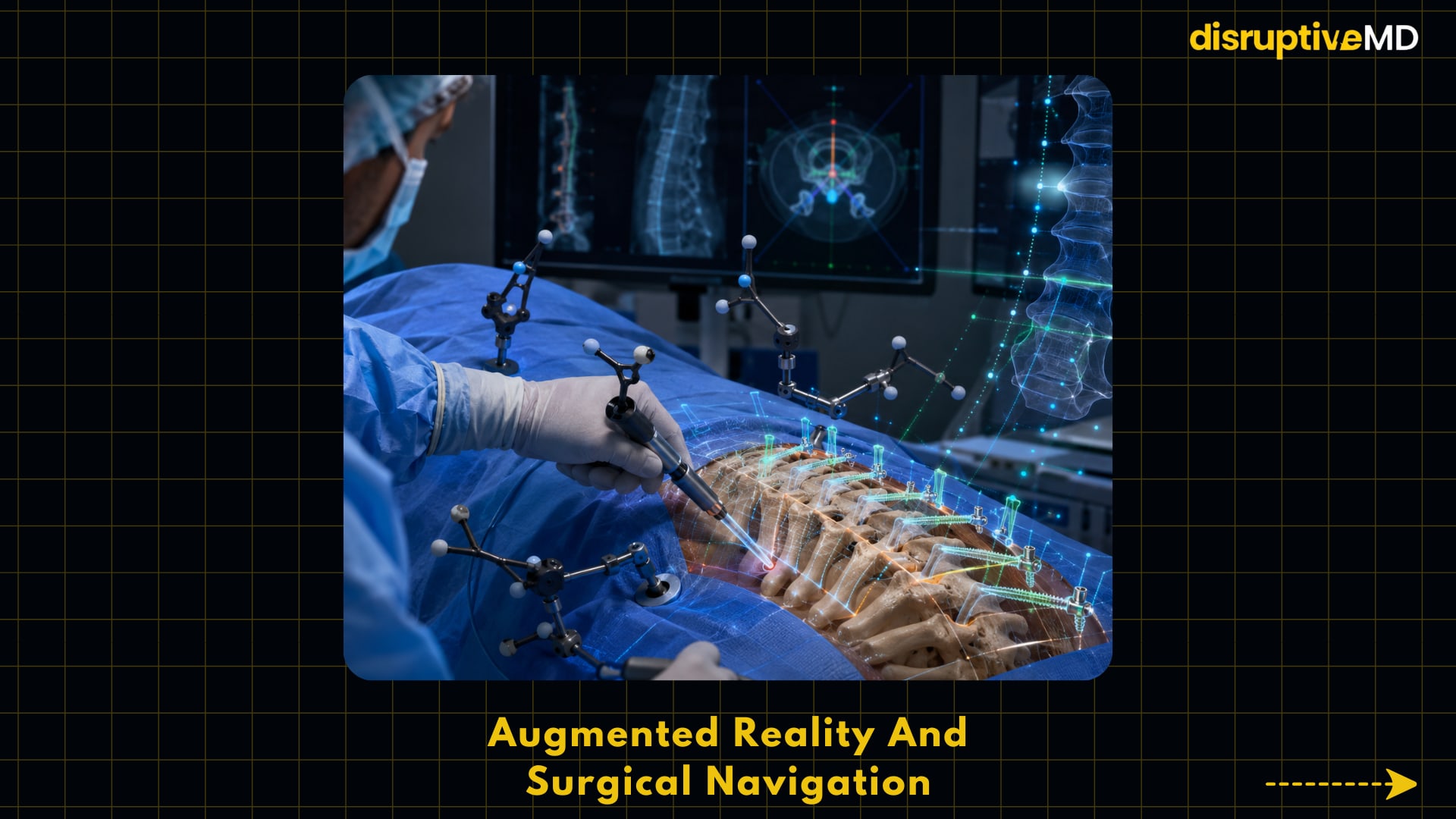
3. Augmented reality and surgical navigation
Augmented Reality (AR) is a technology that superimposes digital information over the real-world perspective of the surgeon commonly via head-mounted displays or navigation devices. AR can overlay the anticipated screw trajectory on the patient’s anatomy in spine surgery, helping to position pedicle screws, the implants that go through strong bony channels in the vertebrae to stabilize the spine. This is important because the margin of error allowed may be small and better guidance may reduce the incidence of misplaced hardware, repetitive exposure to x-rays or the necessity for revision surgery in selected circumstances.
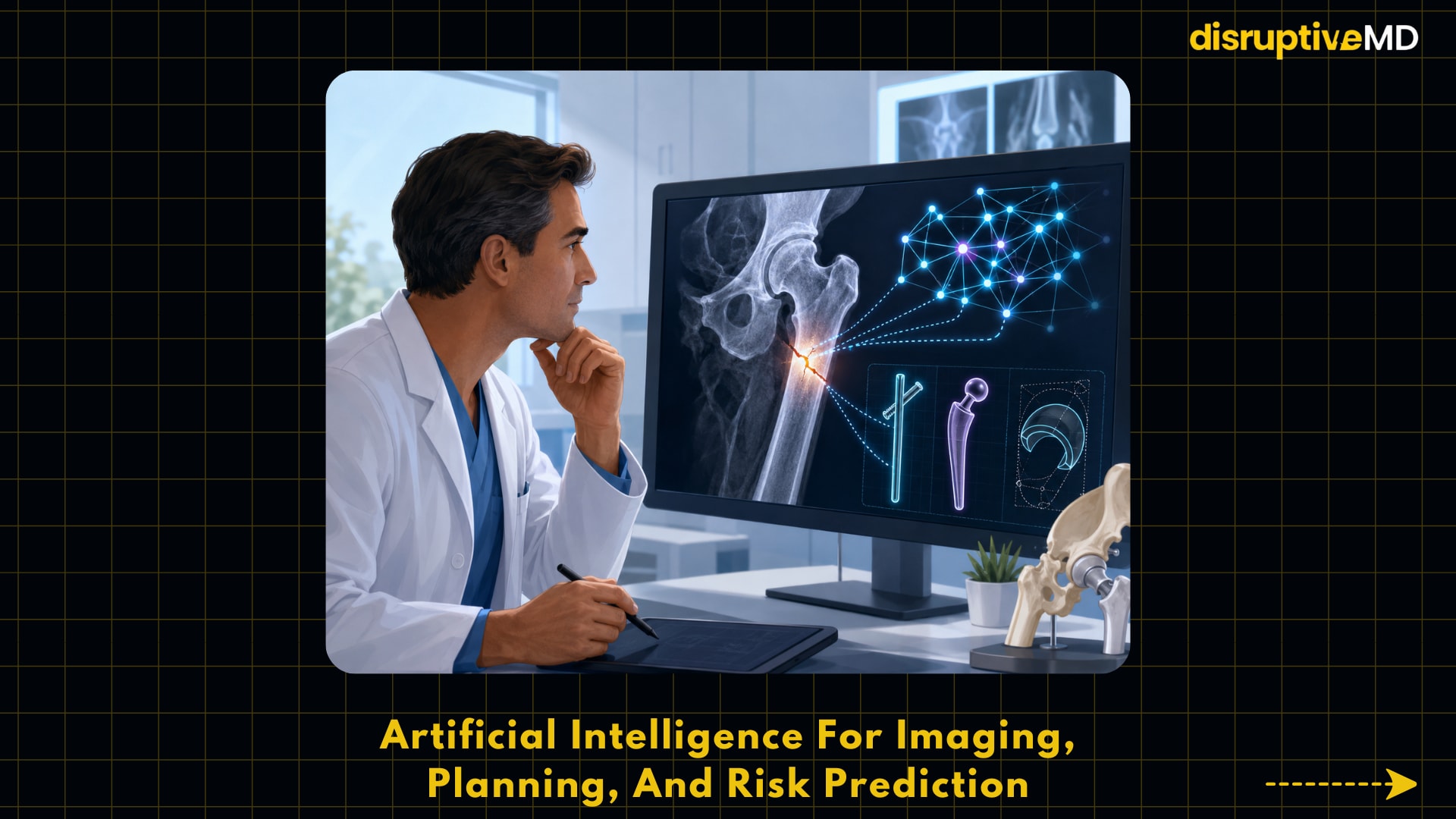
4. Imaging, planning and risk prediction with artificial intelligence
Artificial intelligence in orthopaedics generally refers to machine learning or deep learning in which computer models are trained to identify patterns in x-ray, CT scans, MRI scans, electronic health records, or surgical outcome data. For fracture diagnosis, AI systems can flag questionable areas of radiographs for further inspection by doctors, and for joint replacement, AI can assist with implant sizing, preoperative templating, complication prediction, and workflow planning. This is important, as orthopaedic care is becoming increasingly data intensive and clinical teams need tools that assist, rather than replace, human judgment in image interpretation and treatment planning.
5. Intelligent implants, wearables and connected rehabilitation
Smart orthopedic implants and wearable sensors could provide objective data on post-operative rehabilitation. A sensor-enabled knee implant can capture kinematic data, or data relating to movement such as step count, walking speed, cadence, stride length and knee range of motion. Wearables and smartphone-based rehabilitation systems can be used to monitor exercise adherence and mobility following surgeries such as total knee arthroplasty. This is important since healing is commonly measured in short clinic visits, but genuine recovery occurs over weeks or months at home.
Evidence and Practical Implications
The best evidence for robotic-assisted total knee arthroplasty shows better radiographic accuracy but not yet definitively improved patient-reported outcomes. A systematic review and meta-analysis of 12 randomized controlled trials with 2,200 patients found that robotic-assisted total knee arthroplasty had fewer mechanical alignment outliers than conventional surgery, but had little or no effect on WOMAC patient-reported outcome scores or range of motion. That's essential because, even if the technology seems to improve surgical precision, the more significant clinical question—whether that precision translates into reliably greater long-term pain relief, function, or implant survival—is not yet answered.
The evidence for 3D printed patient specific guidance is good but diverse – the research are different enough that results cannot always be easily merged. A 2025 systematic review of randomized controlled trials in orthopaedic surgery (excluding knee arthroplasty) screened 6310 studies, including 27 RCTs, and found significant benefits for patient-specific guides in several measured domains, especially accuracy and radiation exposure, but only 6 studies were rated as having low risk of bias. This is significant because patient-specific guidelines may have a specialized role in technically demanding procedures, but sweeping claims of superiority require more rigorous, standardized trials.
Some of the best evidence of augmented reality is in spine instrumentation. In a randomized multicentre experiment including 150 patients, the AR-guided pedicle screw insertion was compared with traditional freehand surgery with CT guidance, reporting a full-analysis screw placement success rate of 98.0% in the AR group and 91.7% in the control group. This is important because spine surgery often includes high-risk anatomy and small gains in correct screw placement may be considerable when scaled to a large number of treatments.
AI fracture detection has beyond laboratory curiosity, but works best as clinical decision support rather than an autonomous diagnosis tool. A systematic review and diagnostic-test-accuracy meta-analysis of 17 studies (2024) reported good diagnostic accuracy across most commercial AI fracture-detection systems and anatomical regions and best performance when AI was used with human assessment. This review also reported weaker performance for ribs and spine than many other regions. This is important because AI could help reduce missed fractures and accelerate triage, but physicians still need to check results and know where the model is less dependable.
Connected therapy and smart implants have practical appeal but proof for improved hard clinical outcomes is early. A prospective randomized multicentre trial demonstrated similar postoperative outcomes including range of motion and patient-reported outcome measures for a smartwatch with a mobile app for self-directed rehabilitation after total knee arthroplasty compared to traditional formal physical therapy. A systematic review of wearable sensors after knee arthroplasty reported similar results compared to standard of care in most studies, but also pointed up methodological heterogeneity and the need for longer and more rigorous randomized trials .
Limitations, risks and open questions
The fundamental drawback of robotic orthopaedic surgery is the fact that improved precision does not necessarily translate into improved patient outcomes. Robotic solutions can be more costly, need training, complicate workflow, and not be consistently accessible across hospitals or regions. The existing randomized evidence in total knee arthroplasty suggests improved alignment measurements, but has not yet demonstrated a clinically relevant benefit in pain, function, revision rates or serious adverse events.
The main restriction of 3D printing is quality control throughout the entire digital-to-physical procedure. All of these, imaging quality, segmentation, design software, choice of material, printing conditions, sterilization and post-processing, can have an effect on the safe performance of the final guide or implant. The FDA has released technical recommendations for additive produced medical devices and separate guidance for patient-matched orthopaedic guides, noting the necessity for thorough testing, characterisation, and regulatory uniformity.
The most critical issue with AR navigation is registration inaccuracy, meaning that the digital overlay does not match the patient’s actual anatomy. When the virtual path does not follow the real surgical field it can result in a false sense of security instead of safety. This is the way AR should be seen as a navigation aid at the surgeon's disposal, and not as a replacement for anatomical knowledge, fluoroscopy, CT confirmation or routine safety checks.
The main restriction of AI is generalizability: a model trained on one population, one type of scanner, one hospital workflow, or one fracture pattern, may not perform as well in another. The 2024 meta-analysis on fracture diagnosis showed good overall performance but also vary by anatomical location . It stated that the AI-assisted human assessment generally performed better than the unaided human evaluation in sensitivity . This enables AI as a second reader, not a stand-alone authority.
Smart implants and wearables raise problems concerning privacy, data ownership, digital access, physician burden and clinical effectiveness. The FDA decision statement for one such implantable knee kinematic measurement device notes that the generated data are intended as an adjunct during post-operative monitoring and are not intended to support clinical decision-making or shown to give clinical benefit. This matters because objective data can be useful, but more data don’t automatically enhance care unless physicians know how to analyse and act on it .
Orthobiologics, particularly platelet-rich plasma and stem-cell based treatments, are an area of special caution as they are typically touted as disruptive orthopaedic advancements but have unequal support. The AAOS knee osteoarthritis guideline suggests that platelet-rich plasma may relieve pain and improve function however the recommendation is weak and downgraded because of inconsistent data. The FDA has not approved any regenerative medicine therapy for any orthopaedic problem, including osteoarthritis, tendonitis, disc disease, or back discomfort. This is important as patients may be exposed to commercial claims which are outside the evidence.
Conclusion.
The future of orthopaedic surgery will probably be more digital, more personalised and more measurable but not necessarily better just because it is more technical. Robotic systems and AR navigation may improve technical accuracy; 3D printing may help physicians manage complex anatomy; AI may help with image interpretation and planning; and smart implants or wearables may increase visibility of healing outside the clinic. The most appropriate way to proceed is selective adoption based on patient need, surgeon expertise, regulatory status, cost-effectiveness and outcomes data.
These advancements are important for individuals and health systems since orthopaedic disease affects mobility, independence, employment and quality of life worldwide. For clinicians and researchers, they set the bar higher. New tools need to demonstrate not only that they are accurate, but that they enhance safety, function, durability, equity, and real-world care delivery.
Evidence Level
Limited/mixed evidence. Some of the technologies presented here are regulatory cleared or supported by randomized trials for certain applications, like robotic alignment, AR-guided screw placement, AI fracture detection, and wearable-assisted rehabilitation. However, the evidence is variable depending on the surgery, technology, anatomic area, period of follow-up, and patient demographic. Better accuracy or surveillance is the dominant current theme, although long-term dominance in patient-cantered outcomes is unclear for many applications.
Educational Disclaimer
This text is for educational purposes only and is not a substitute for professional medical advice, diagnosis or treatment. When considering orthopaedic surgery, implants, rehabilitation or regenerative therapies, decisions should be made in collaboration with trained healthcare specialists who can analyse the specific patient’s condition, risks, goals and the available evidence.
References
- World Health Organization. Musculoskeletal health: fact sheet.
- American Academy of Orthopaedic Surgeons. Robotic-assisted joint replacement.
- Ruangsomboon, P., Ruangsomboon, O., Pornrattanamaneewong, C., Narkbunnam, R., & Chareancholvanich, K. (2023). Clinical and radiological outcomes of robotic-assisted versus conventional total knee arthroplasty: a systematic review and meta-analysis of randomized controlled trials. Acta Orthopaedica, 94, 60–79. https://doi.org/10.2340/17453674.2023.9411.
- U.S. Food and Drug Administration. 3D printing of medical devices.
- Kampkuiper, N., ten Heggeler, R., Nellensteijn, J. et al. Clinical added value of 3D printed patient-specific guides in orthopedic surgery (excluding knee arthroplasty): a systematic review. Arch Orthop Trauma Surg 145, 173 (2025). https://doi.org/10.1007/s00402-025-05775-2.
- U.S. Food and Drug Administration. Patient-matched guides for orthopedic implants: guidance for industry and FDA staff.
- Ma Y, Wu J, Dong Y, Tang H, Ma X. Augmented Reality Navigation System Enhances the Accuracy of Spinal Surgery Pedicle Screw Placement: A Randomized, Multicenter, Parallel-Controlled Clinical Trial. Orthop Surg. 2025 Feb;17(2):631-643. doi: 10.1111/os.14295. Epub 2025 Jan 15. PMID: 39815419; PMCID: PMC11787979.
- Husarek, J., Hess, S., Razaeian, S. et al. Artificial intelligence in commercial fracture detection products: a systematic review and meta-analysis of diagnostic test accuracy. Sci Rep 14, 23053 (2024). https://doi.org/10.1038/s41598-024-73058-8.
- Tripuraneni K, Foran J, Munson N ... A Smartwatch Paired With A Mobile Application Provides Postoperative Self-Directed Rehabilitation Without Compromising Total Knee Arthroplasty Outcomes: A Randomized Controlled Trial The Journal of Arthroplasty, 2021; 36, 3888-3893.
- King SW, et al. Wearable sensors to guide remote rehabilitation following knee arthroplasty surgery.
- U.S. Food and Drug Administration. De Novo decision summary: Canary Tibial Extension with CHIRP System.
- U.S. Food and Drug Administration. Important patient and consumer information about regenerative medicine therapies.